

Abstract
Aim
Healthcare is recognized as a productive field of research today. Due to the fact that nurses are stressed physically and emotionally, reducing burnout among nurses is an important research issue. The purpose of this paper is to explore clinical nurses’ experiences and perspectives of living with burnout using qualitative studies
Method
A systematic searchwas explored, using CINAHL, MEDLINE, EMBASE, British nursing Index, ASSIA and PsycINFO on clinical nurses burnout and the consequences of it on nurses health. Hundred articles were retrieved out of which best 10 articles were selected. This was done by reviewing most reliable articles for study of which first selection was to compare title and abstract where some articles were excluded and second selection was by reading the full articles where most suitable articles were selected and evaluated for the methodological short comings.
Findings of the review
The major findings established were, unsupportive management by giving vast negative perceptions about the nursing management potentially leading to staff burnout. Nurses’ also experienced lack of recognition, encouragement, support, poor supervision, high expectation from nursing management and unsupportive administrations.
Conclusion and recommendations
Findings suggest that nurses’ working under heavy workload and pressure experiencing high level of burnout affecting them mentally and physically, consequently leading them to move out of the industry or with a low performance in their work. Thus health care organisations should be more cautious about staff satisfaction and their wellbeing in order to restrain nurses. Additionally it is vital for the supervisors and nurse managers to conduct supervisory sessions and meetings to consider nurses’ problem and to assess their workload.
INTRODUCTION
The term “Burnout” which appeared around (1975) in scientific literature, is referred as a low job satisfaction in many cases (Lauderdale,1982,p35). There is no specific definition for burnout in terms of medical condition, but it is well recognised and defined as a psychological condition. As a matter of fact burnout is said to be the final stage of stress when everything else fails (Intermission care and rehabilitation society (IMCARES), 2008 [online]). Thus, according to Reddy (2007 p20) burnout is a state of physical, mental and psychological exhaustion with depersonalization and a reduction of personnel accomplishment caused by prolonged exposure to stressful work situations. It reduces work performance and result in failure of professionalism (Reddy 2007, p20). Maslachet al (1996) stated that, emotional exhaustion is the depletion of emotional resources, depersonalisation refers to the negative feeling and attitude about others along with reduced professionalism and personnel accomplishment is the negative feeling about own self, especially on work area (Maslachet al 1996 p4 cited in Patric & Lavery 2006 p43). Where else, according to Cochihov and Briebart (2000 p308), the most common outcome which is used to measure stress is burnout, characterised of progressive loss of idealism and energy experienced by people in helping professional as a result of their work condition. For the purpose of this review burnout was referred as low job satisfaction and traumatic stress.
Table 1.13
.png)
Nurses experiencing burnout: An important issue to be considered
Comparatively health care professionals are at higher risk of getting burnout than any other profession, because of the nature of their work (Erikson & Grove 2008) and as well as the life and death decisions they take (Potter 2005, [online]). The main reason why nurses move out of the industry is because they experience stress,sadness, powerlessness, exhaustion, and frustration as their daily routine (Erikson & Grove 2008). From a health care commission report on Maidstone and Tunbridge wells NHS (National Health Service) revealed that staff shortage, ill health and heavy work load are contributory factors for failure of effective dealing with the patients. In addition staff are also unaware of their own wellbeing for the safety of the patients (Bence 2008, p28). This shows that there is a link between nurses’ burnout and patient satisfaction.
Nurses also present high mortality rates, stress related diseases, elevated blood pressure, anxiety and depression with suicidal attempts. This further leads to increased rate of mistakes and job injuries, consequently affecting the quality of care provided to the patients (Salmond and Ropis 2005 p301). A Nursing Times survey, conducted on 2000 nurses revealed that seven out of ten suffered from work related stress, where sick leaves were increased by 30 or more sick days for the previous years as a result of job threats, increased workload and staff shortage (Jones 2007).
In addition to this, another survey carried on 2007 by the health care commission of NHS(national Health Service) identifies thirteen percent of staff were physically attacked by their patients or relatives, eight percent of staff were reported of harassment and bullied by the managers and thirteen percent by their colleagues (Bence 2008 p28).The level of bullying and harassment has increased in the past six years and most of all it is existing from the line of mangers (Paton 2006).
Consequently nurses’ negative feelings towards their job, mixed with their feeling of burnout are influenced by organisational practices of work environment. (Aiken et al 2002, 1997cited in Erikson & Grove 2008). Supporting to this a national sample survey indicated that nurses job satisfaction is influenced by the structure of the job than the composition of work (Erikson & Grove 2008).
Consequences of burnout
Burnout in nursing effects not only the organisation but also to the patients as well as the nurses’ well being. As a result of burnout, nurses’ job turnover has been increasing day by day. Newly graduates job turnover has been increased by less than 3 years. Thus, this decreased in staff level add more pressure to experienced staff presently working. In addition to this under resources has shown a significant level of staff burnout in many studies and effects adversely on patient outcome and also effecting nurses emotionally (Currid, 2009, p40-46).
Prolonged exposure to stressful situations and burnout leaves the nurses with low job satisfaction. In addition to this when there is no support from management as well as from the working colleagues, nurses are left with emotional and physical exhaustion (Bush 2009 ).
All these things consequently leads to a low morale, high absenteeism, high job turn over and other personnel conflicts and thereby reducing the job satisfaction causing low performance in work ( Carson & Fagin 1996, Cited in Fothergill & Hannigan 2000).
At the same time, when there is a staff shortage, it affect the organisation badly which sometimes lead to health care service changes, hospital closures, low morale within the organisation and poor atmosphere (Fothergill & Hannigan 2000).
Gap within the literature
Although many studies have been done on the topic “burnout”, there are fewer studies done on nurses’ burnout and also the studies done are mostly on to a specific clinical area. A preliminary search through chochrane library shows only two reviews of the topic and it is also about professional burnout. Moreover, using databases like British nursing index, CINAHL (Cumulative index to nursing and allied health litrature), Medline, AMED( Allied and Complementary Medicine) and psychINFO, shows that most of the systematic reviews were on stress, nurse turn over and specifically onto areas like cancer or mental health nurses. Furthermore, TRIP database, Pub med and CRD was also explored for any reviews on the topic area, where it gave almost similar results as chochrane and other databases. Most of the topics were on health professional burnout, stress and job satisfaction.
Beside from this, a literature review by Edwards et al (2000 p7-14) was similar review done on the issue of burnout, but it was focussed on community mental health nursing as evidenced from title itself and not focussed on clinical nurses. Similarly another research study by Patrick and Lavery (2006 p43-47) on “Burnout in nursing” was similar to the topic chosen but was focussed onto nurses’ generally and not specifically to clinical nurses. Most importantly, the study was not a systematic review as it was clear that the study design was randomised survey (Patrick and Lavery 2007 p43). Consequently, a gap within literature for a systematic review exists, with valuable information for nurses working on clinical care setting, highlighting devastating effect on their personnel health and importance of early recognition of it for effective coping strategies.
METHDOLOGY
According to the inclusion and exclusion criteria table 5.11 represents the standardised form as highlighted in the protocol for the selection process. Further this approach was used throughout the selection process for the reliability of the process.
Table 5.11
Inclusion and exclusion criteria form for the selection of study
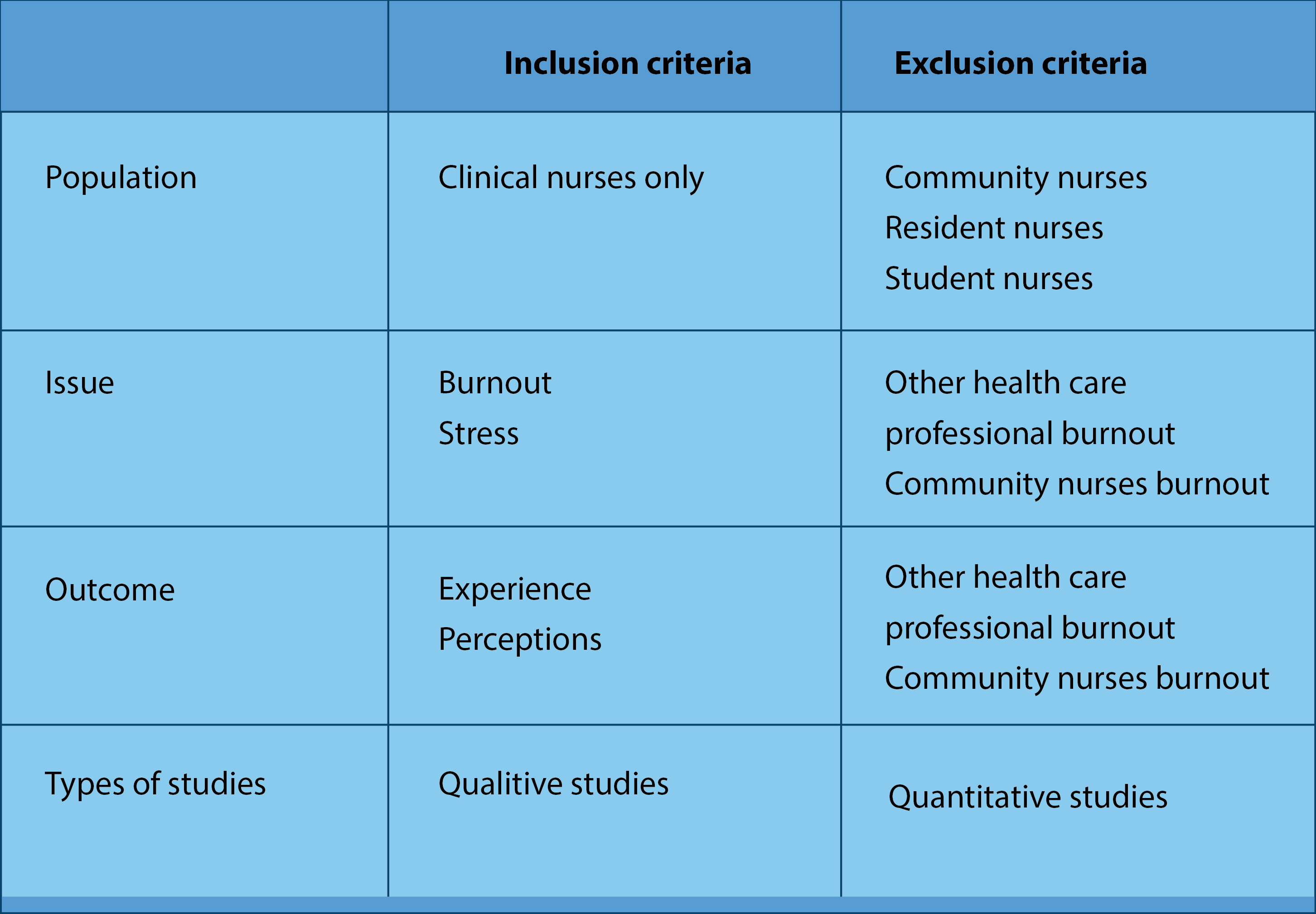
The first selection was undertaken using a standardised form including three options; yes, no and unsure, for which studies scored with a yes or an unsure were taken for the next section of reading the full paper.
Within this section all the papers retrieved from the comprehensive search process was further looked into its tile and abstract with regard to inclusion and exclusion criteria of the PIO elements from the question. In addition, as mentioned before a second researcher was involved in the selection and derived almost the same conclusion within the criteria of the standard form apparent from. Eighty six papers were retrieved from this section and were taken for the next selection out of which the discarded papers failed to achieve the inclusion criteria provided in the template.
McMaster frameworks provide with basic terms, which is easy to follow and could be used by clinicians, students and researchers with proper guidance in evaluating qualitative as well as qualitative designs (Law et al 1998).
All the papers were individually evaluated using the McMaster evaluation form with a second reviewer. During this stage of evaluation, for an in depth understanding of papers the McMaster form was modified into methodological quality.
Table 5.31

Using Mc master evaluation form, all the ten papers selected were further evaluated for its similarities and differences, where overall quality of the papers were established.
Overall all the papers have established most of the elements of credibility except seven and eight. However papers two, four, five six and ten have achieved a good credibility in relation to the elements of it.
A contextual documentation includes, field note from observation, interviews conducted, participants study setting and locations. This method was apparent in papers, one two, three, four, five, six , eight , nine and ten. Secondly methodological documentation gives a rational for the chosen design and this is apparent in papers one, two , three, four, five, six, seven , eight and ten. Thirdly personal response is the self awareness of the researcher on the process and this was apparent in papers one, two, four, five and six. Finally analytical documentation gives the reflection of the researcher and a theoretical insight upon analysis where in papers one, two, four, five, six, eight and nine this was apparent.
All the studies included were conducted in foreign countries and therefore, the health care system and the participants involved may face different experience in other countries.
Following to McMaster approach, methodological quality of all the ten papers were established in light of the original form. Further the questions in the form were changed from 20 questions to 44 questions. A numerical aspect was established in evaluating the studies where 2 was given for yes and 0 for no. additionally, a scale was used to measure the qualities of the papers form poor to very good. Within this process also a second researcher was used in evaluating the papers, further minimising researcher bias for which no disagreements were raised.
All ten papers were initially analysed by reading and reading it several times to fully immerse into data. During this process similar phrases and terms were noted from all the papers and memos were made. All the memos were compared for similarities and differences. This was again further explored by a second researcher and emerging themes were compared, consequently deriving four main themes which are presented in table 5.91.
Table 5.91

After this process, a discussion was held with second researcher and it was agreed to extract similar data from all the studies under the emergent themes and again to develop subthemes. Furthermore, the subthemes emerged from this stage were explored focusing onto most frequently occurring themes within all papers. Within this process two new themes were again emerged which is presented in table 5.92
Table 5.92

yet again all the papers were read and re read to extract data under the developed themes and colour codes were given to identify the themes. The standard form apparent from protocol for data extraction was applied to extract data , table 5.93 represents the colour codes given to each theme.
Table 5.93
Derived themes with relevant colour

Final data was extracted, noting page numbers, columns and line numbers for quick check. Highlighted colour coded data were then transferred to data extraction forms under the relevant themes with subthemes in relation to each theme.
Having derived themes with the relevant subthemes, for the consistency of the study independent evaluation with second researcher was again conducted. Extracted data from all studies were narratives since it was a qualitative design.
RESULTS
Original question of McMaster questions were changed to 44 questions covering all the section of the framework. This was marked in a numerical format, where 2 represents a “yes”, 1 for not addressed and 0 for “no”. Furthermore, this was transferred into a scale for a comprehensiveness of the results, where scale measures form 1 to 5 with, 1 very poor quality, 2 for poor, 3 for an average, 4 for good quality and 5 for a very good paper.
Table 6.11
Results of the systemic search

Over all methodology of the papers was assessed using McMaster framework. This was further modified in order to establish a scoring system for the papers to assess the best evidence synthesis
Keys
2 = Yes
1= Not addressed
0 = No
From the table above quality of the papers were added and scored on the scale below from 1 to 5

1. Score under 20 is very poor quality paper
2. 20- 44 is considered as poor quality paper
3. 44- 60 is average quality paper
4. 60 – 75 is a good quality paper
5. Over 75 is scored as very good quality paper

Final stage of the review also known as synthesizing is the process which explicit the findings for data extraction in relation to all paper findings.
In order maintain rigour of the study the related key words were double checked with the literatures for the similarities and differences. Further it was explored in comparison with the summaries of each paper where it gave the same result of themes. Derived themes and the subthemes were presented in Table 6.51 and data extraction form was attached to appendix 4 for further exploration of the process. This would also give an insight of the initial idea and thoughts during the process which would be apparent in appendix 3.
Theme one: experience of unsupportive management
Five out of ten papers covered this theme of having unsupportive management by giving vast negative perceptions about the management potentially leading to staff burnout. This theme was supported by nurses’ perceptions and experiences of negativism towards their work, lack of recognition, encouragement, support, poor supervision, high expectation from nursing management and unsupportive administrations.
One of the participants expressed her feeling as:
“I feel like it’s something that always hangs over me. And then there’s this with management, not being seen or acknowledged by supervisors, it really affects me. It’s not exactly staff-friendly I don’t think”.
Olofsson and Bengstsson and Brink (2003, p334 col 1 lines13-17)
Most frequently apparent issue from all ten papers were, unnoticed heavy workloads which were not recognised neither supported by the supervisors and lack of emotional support. This was an important and a common issue to bring into nursing managers consideration for the motivation and job satisfaction of the staff.
"Management is not particularly helpful you have to solve the problem yourself .They listen to what is happening and are aware, but don't actually feel the anxiety or the stress experienced by us."
Murphy (2004, p 427, col 2 , lines 5-9 )
Another frequent concern issue for the nurses were poor supervision by the supervisors which supported the above highlighted issue of lack of recognition of work performance. Nurses’ had described this issue for not receiving any feedback from them, either negative or positive, leaving them confused and stressed.
In light of the papers, it was apparent that nurse management plays an important role for nurses’ job satisfaction and motivation. Appreciation and acknowledgement by their supervisors for it could motivate them and gain job satisfaction.
Theme two: physical and psychological aspects:
9 out of 10 papers supported this theme as it was apparent from the question itself that issue under investigation was a psychological consequence of workplace distress. Most frequently expressed psychological consequences from all of the papers were frustration, hopelessness, powerlessness, helplessness and emotional exhaustion. These characteristics were apparent in the background section and were frequently occurred throughout all the papers. Each of the concept was further been explored in relation to the described narration of the nurses.
Hopelessness was described form paper 1 as, having no influence over the work situation which further lead to loss of commitment in their work, feeling hopeless and poorly account for their heavy workload.
One of the nurse stated:
“We talk every day about our situation at work, we do. Then you feel hopelessness. It feels like you can’t do anything about it”.
Olofsson and Bengstsson and Brink (2003, p335 col 2 lines48-50)
Frustration was another frequently occurred concept under the theme which was apparent from almost all the nine papers. Not having enough time to care for patients, receiving insults over which they don’t have influence, asking relatives for help because of their heavy workload and disrespect from patients, family, doctors and superiors made them frustrated about the situation.
“The public don’t respect nurses anymore. I know of a colleague who was attacked at a taxi rank by the family of a patient because they said she wasn’t giving him proper care. People don’t recognise the nursing profession as being noble as they did in the past. I can’t dare to wear my nurse’s uniform when I go home. Before leaving the hospital, I remove my epaulettes; so that people can think I work for Pick ‘n Pay [a food chain store] or something. I’m proud of being a nurse, but it is risky these days to say that you are one. People think because we work with HIV positive people, that we are contaminated or something”.
Smit ( 2005, p26, col 1, lines 36 -45 )
Powerlessness was another leading concern for the nurses’ for they do not have influence on their working environment. They felt powerless when they do not have enough time and they were not encouraged to involve in medical care decisions.
“But I still think in a way, I’ve complained several times but it’s not taken seriously. It’s swept under the rug. So then it really feels, what you say, it’s not worth much. In the long run I don’t think this is good for people. You need to feel involved and that you can change things”
Olofsson and Bengstsson and Brink (2003, p355 col 2 lines 16-21)
From papers one, five, eight and ten it was apparent that participants were physically exhausted suggesting symptom of burnout. From paper five the apparent physical symptoms were anger, insomnia, tiredness and irritation leading to physiological exhaustion, consequently resulting in job turnover.
“In other situations, the outcome was that of being ‘‘overwhelmed’’ with resultant ‘‘bad’’ feelings about the job, anger, difficulty sleeping, questioning their ability, and a dread of returning to work. The resulting emotional and physical exhaustion was reported by all RNs with no identified methods of coping, other than ‘‘rest’’ and ‘‘getting away.’’
Hall (2004, p 12, col 1 , lines 47 – 54 )
Theme three: Inadequate availability of resources
This theme was supported by paper one, two, three, four, five, seven and eight. Inadequate availability of resources mainly highlighted within the studies were, inadequacy of staff, time, high responsibilities with limited resources, skilled staff and basic resources for preventive measures.
Mostly from all, from the mentioned papers most common issue highlighted was inadequacy of staff with limited resources.
“Management has forgotten what it’s like working in the wards. How can they expect us to provide quality care if there’s not enough hands to help, if there’s not enough medication available, if there’s not enough clean linen for the patients’ beds? I ask you?!”
Smit ( 2005, p26, col 2, lines 23 -26 )
The unit was expanding very quickly and they were very short staffed, and we were working twilights and days in 7 week, which left everyone feeling totally exhausted, the staff were getting ill. I myself ended up with pneumonia. I just felt so run down."
Murphy (2004, p 426, col 2 , lines 30-36 )
Theme four: experience of work alienation
This theme was supported by paper two, five and eight, for the unfamiliar work environment and equipments, inexperience and incompetency in work and lack of knowledge.
Unfamiliar work environment and equipment was a common issue under this theme. Difficulty in handling the advance equipments and operating the new machines were a time consuming for them as they do not have the proper guidance and exposure to it. This issue was mostly apparent in paper 2.
The issues of unfamiliar work environment and lack of knowledge was mostly due the lack of experience and information about work environment which caused frustration.
“They have got ever so many pieces of advanced equipment, monitoring equipment. But they don’t understand them very well; they are not good at controlling all the machines. So they really hope that they can have more lessons and study more about these electric machines, to get more knowledge”.
Tang, Johansson, Wadensten, Wenneberg and Ahlstro¨m (2007, p815, para-2, lines 6-9)
Theme five: Experiencing excessive and heavy workload
This theme was supported by all the papers except paper two. Therefore this issue was considered to be the most leading issue for staff burnout out of all the issues, since the majority of the papers cover the theme. This was highlighted in papers as multitasks with frequent interruptions within a limited time or performing multiple interventions at a limited time which further causes staff fatigue and exhaustion.
“You never get any peace; never get done with anything, always interrupted by ringing telephones. During all this an assistant nurse comes and some patient is ill and you have to run. Then run from that to talk on the phone with a relative who’s calling and worried. Then rounds have to be done. These constant interruptions. While I’m supposed to do these things I want to get out and see the patients, what am I sitting here and documenting? How is the patient? How is he or she really feeling?”
Olofsson and Bengstsson and Brink (2003, p354 col 2, lines 39-52)
From paper five it was apparent that nurses performed seventeen multiple interventions within fifteen minutes of observation by the researcher, and it was also highlighted that they had to perform task for which an unskilled labour could do, causing additional pressure.
“The simple things like turning a patient every two hours in an acute-care setting . . .if we could have two techs to maybe come in instead of me going in and either doing it myself, which I don’t have time, or assisting a tech to do it when I’ve got several other things that are more of a priority like giving meds or a patient going bad or you are watching a patient. . ”
Hall (2004, p10, col 1 lines 26-32)
Theme six: strategies for coping mechanism
This theme supported five out of ten papers, providing perceptions of and experiences of how they relived and coped with the stressors faced within the care setting. Apparent strategies from the papers were; attempting to reduce stress by remaining calm and quite during the stressful situations, relieving by individual interests, using support and assistance from peers and family members, communicating with co workers, getting involved in something else ignoring the situation and reflecting back the situation and communicating with a colleague.
“When you’re sad, it helps if they are gentle and don’t keep telling you ‘Do this’ or ‘Do that’ but tell each other instead ‘Don’t disturb her she’s feeling miserable”.
Boroujeni, Mohammadi, Oskouie and Sandberg (2008, p 2334, col 1, lines 34-36).
Various types of coping mechanisms were apparent from paper eight specifically including alcohol consumption, smoking, drinking with friends and doing things of interests. This paper also highlights recommendations to cope with stress.
In summary of all the themes derived, it enhances a clear insight of nurse’s experiences and perception of burnout, further achieving the objective of the study. As mentioned in the chapter two bringing these issues into health care consideration would reduce nurses turnover, promote job satisfaction and increased quality care further benefiting the organisation and well being of nurses.
Furthermore the study established a good in depth description in understanding the subject under phenomena by exploring the key components of burnout. Additionally it gives a vast differences and similarities of experiences with different levels of burnout from each group of nurses. As apparent from almost all the papers the most frequently occurred issues were established in theme two and five; psychological consequences and heavy workload which has to be taken into consideration.
CHAPTER SEVEN: DISSCUSSION
This chapter would consist, ethical issues, preliminary synthesis of findings with regard to included studies, comparison of data emerged within the study in relation to the study background, methodological shortcomings of the selected ten papers , limitations of study, recommendation and conclusion.
Major findings established within the review were unsupportive management, oppressive workloads, and experiences of physiological and psychological aspects, work alienation and strategies for coping mechanisms to overcome stressful situations. As the aim of the review was to explore nurses’ experiences and perceptions living with burnout, from the findings it was evident that nurses are deeply involved in stressful situations while in clinical areas which consequently lead them to burnout. Additionally from the initial definition of burnout three major concepts were apparent consisting of psychological and physiological exhaustion, depersonalisation and personal accomplishment which further describe the defining attributes of burnout in relation to the findings. Apparently almost all the findings were related to the study background achieving the aims and objectives of the study.
In relation to the initial background, it was apparent that emotional exhaustion as a consequence of unsupportive management and bullying and harassment arising from the line of managers which supports the findings of the review. Secondly in the epidemiology it was highlighted that oppressive workload further leading to emotional exhaustion. Psychological and physiological aspects consequently leads to stress , sadness, powerlessness, exhaustion further leading job turnover and high absenteeism was also apparent from the background literature. Thirdly work alienation was described as inexperience or lack of skills and knowledge which was also highlighted in the epidemiology of the background with lack of resources causing exhaustion and fatigue further leading to ill health. Findings show some of the coping strategies highlighted in the background to relive their stressful situations.
Almost all the paper findings gave similar results for the experiences in stressful situations and were all negative experiences except for two papers. It was interesting that these two papers gave both negative and positive experiences and perceptions. One paper expressed empathy as a compassion and self fulfilment as rewarding for their care being appreciated and the other paper addressed to added income with health insurance and flexible working hours. However they also experienced same stressful situations with these benefits.
In relation to the findings of this review to the other authors, the most significant finding was unsupportive management for which majority of the papers included lack of support, recognition and acknowledgement from supervisors. Supporting to this Severinsson and Kamaker (1999 p88) highlighted the importance of clinical supervision for the imbalance of work demands and nurses’ inability to handle it due to moral stress. Additionally it was apparent from their findings that nurses’ needs to support their personal qualities of development via self awareness and integrated knowledge. This finding also supported the finding from the review for work alienation which was described as lack of knowledge and inexperience of the nurses. As in Serverinsson model of nursing supervision, it is important for the nurses to have opportunity to discuss their own problems and experiences in clinical nursing supervisions (2001 p43). Apparently this model supports the existing theory for the implementation to practice.
Another major finding from the review was physiological and psychological issues including powerlessness, hopelessness, exhaustion, frustration and physiological impairment. Physical symptoms associated were headache, palpitation, fear, muscle pain, and tiredness in associated finding of Koponen and Freden ( 2005 p 23). Another finding represents powerlessness of the nurses as lack of control over the practice and having little influence over their daily practices (Attree 2004 p 393) giving similar findings as the review findings. Heavy workload and frequent interruptions were also a common findings evident form papers for which findings of salmond and Ropis (2005 p 307) supported this by medical- surgical nurses competing the workload by frequent interruptions including phone calls , personnel needing assistance, emergency priorities leading them to tiredness and exhaustion. Another similar study findings to the review was Inadequate resources for which Taylor and Barling (2004 p122) gave similar findings of lack of resources including staff and time. In accordance to the findings of KJerulf, Popova and baker (2004 p 434) provides similar findings coping strategies to cope by concentrating on the task and ignoring the situation.
Thus, as evident from the literature finding and the review findings, a major concern of the nurses’ were lack of managerial support, further placing a question upon the rationale of unsupportive management or the nurse managers. A need of a study on this particular issue exists to further explore the rationale behind nurse managers’ attitude towards clinical nurses.
Ethical considerations
As the nature of the issue explored, included a high level of critiques to nursing management for the improvement of organisation, it was apparent from the papers that some nurses were reluctant to discuss the issue since it involved higher management and for the fear of breaching their autonomy and confidentiality. Thus it is important to reassure participants’ that identity is protected and the data collected would not be released to any third parties (Ryan, Coughlan, Cronin 2007 p738). It is therefore important to gain an informed consent, for it protects the autonomy and confidentiality under the five human rights of ANA guidelines (Mancee and McCabe 2008 p146). Further the three fundamental ethical principles of autonomy, beneficence and justice should be maintained.
Therefore all the papers should address to the issue of confidentiality and gained informed consent, right to withdraw from study at any time (Mancee and McCabe 2008 p152) with an authorization approval from an ethical board. In light of the selected ten papers, all the papers obtained an informed consent and an authorization approval except paper nine. For not addressing a gained informed consent, it has failed to uphold the standards of ethics (Mancee and McCabe 2008 p146). This further would have an effect on the study findings since it impacts trustworthiness of the study. Only three papers had addressed to right to withdrawal from the study at anytime. However only paper six addressed to all components including, revisiting throughout the duration of the study, ensured participants that their rights were protected and have the right to withdraw at any time, being informed about the study purpose with research procedure.
Thus, questions were raised upon participants’ awareness of the study and their protection being maintained which further creates an ethical dilemma upon the studies.
Limitations of the review
Study was focussed on to clinical nurses including all the areas of hospital care setting and areas such as operation theatre, labour room, gynaecology, paediatric and oncology were not searched, which would have an impact on study findings of the review.
Recommendations and conclusions
As highlighted before nurse managers and management needs to have a closer look onto the nurses’ job satisfaction, considering their physiological and psychological needs. It is important to Recognise and acknowledge their work performance in staff motivations. Nurses should be encouraged and given opportunities for further studies to enhance their knowledge. Education on coping strategies would be further beneficial for the preregistration in preparation for the carrier as well as post graduates to cope with their stressors.
Findings suggest that nurses’ working under heavy workload pressure experiencing high level of burnout affecting them mentally and physically, which is a serious issue to consider. Consequently this leads them to move out of the industry or with a low performance in their work. Thus health care managements should be more cautious about staff satisfaction and their wellbeing in order to restrain nurses. Additionally it is vital for the supervisors and nurse managers to conduct supervisory sessions and meetings to consider nurses’ problem and to assess their workload. Within the light of this review nurses’ should be able to identify and recognise their stressors early in order to prevent them from burnout or post traumatic stress. Moreover nurses should focus on their own health and well being, caring for themselves which would consequently decrease the level of burnout and promote a quality care. Also management should provide nurses with educational opportunities for further learning and development of their skills.
Reference list
Attree M (2005) Nursing agency and governance: registered nurses’ perceptions Journal of Nursing management (13) 387- 396
American Nurses Association National Database of Nursing Quality Indicators 2008 Available @ [onine]:
http://www.nursingworld.org/MainMenuCategories/ANAPoliticalPower/Federal/Issues/safestaffing.aspx
Accessed on: [2nd October 2009]
Brown C J (2009) Self- renewal leadership: The lived experience of caring for self Journal of Holistic nursing 27(2) 75-84
Bouroujeni A.Z, Mohammadi R, Oskouie S.F.H and Sandberg J (2008) Iranian nurses’ preparation for loss: finding a balance in end- of life care Journal of clinical nursing 18,2329-2336.
Bayer D C and France N E M (2008) The lived experiences of registered nurses providing care to patients with dementia in the acute care setting : A phenomenological study International journal of human caring 12(4) 44-49
Bowling A and Ebrahim S Handbook of health research methods: investigation, measurement and analysis (2005) England Bell and Bain ltd.
Burns N and Grove S K The practice of nursing research: conduct, critique, and utilization 5th edition (2005) Philadelphia Elsevier Saunders
Bence, A. (2008) Come on, get happy Nurse entrepreneur on personal fulfilment – hers and yours. NMC News issue 26 /October ,London.
Avalable at: [online]
http://www.nmc-uk.org/aArticleSearch.aspx?SearchText=burnout
Accessed on [ 22nd September 2009]
Bush N.J. (2009) Compasion fatigues : Are you at risk? Oncology nursing forum . 36(1) 24-28.
Currid T (2009) experiences of stress among nurses in acute mental health settings. Nursing standard 23 (44) 40 – 46
Center for Reviews and Dissemination, university of York 2008, (2009) Systemic reviews CRDs guidance for undertaking review in health care York publishing services limited Layerthorpe.
Cochinov .H.M and Breibart W ( 2000) Hand book of psychiatry in palliative medicine Oxford university New York
Debra S(2004) Work related stress of Registered nurses in a hospital setting Journal for nurses in staff development 20(1) 6-14
Edwards D, Bunard P, Coyle D, Fothergill A and Hannigan B (2000) Stress and burnout in community mental health nursing a review of literature Journal of psychiatry and mental health nursing vol:7, p7-14
Erikson, J. R & Grove, C.J.W (2008) Why emotions matter: Age, agitation, and burnout among registered nurses. Journal of American nurses association, vol:13 January USA
Firmin M W and Bailey M (2008) When caretaking competes with care giving: a qualitative study of full-time working mothers who are nurse managers Journal of Nursing Management 16, 858–867
Gillespie M and Melby V (2003) Burnout among nursing staff in accident and emergency and acute medicine: a comparative study Journal of Clinical Nursing vol. 12: p842–851
Glaser B G and Straus A L ( 1999) The discovery of grounded theory: strategies for qualitative research Aldine New York
Gray,J.A.M. (2001) Evidenced based Healthcare: How to make Health policy and management decissions 2nd edition, Llondon, Churchill Livingstone.
Houser J (2008) Nursing research and creating evidence, Canada Jones and bartelette
Holloway I and Wheeler S (2002) Qualitative research in nursing 2nd edition United Kingdom Blackwell publishing
Koponen S B and Freden L ( 2005) long term stress, burnout and patient- nurse relations: qualitative interview study about nurses’ experiences Scand Journal of caring Science (19) 20-27
Khowaja K, Merchant R J and Hirani D (2005) Registered nurses perception of work satisfaction at a Tertiary Care University Hospital Journal of Nursing Management 13, 32–39
Khan, Kunz, Kliejnen and Antes (2009) Systematic Reviews to support evidence-based medicine: How to review and apply findings of health care research. United Kingdom, Royal society of medicine press ltd.
Jones,E.V. (2007) Stress: why are nurses’ anxiety levels rising? The healers Nursing Times 103(27)16-17
Laverty S M (2003) Hermeneutic phenomenology and phenomenology: A comparison of historical and methodological considerations International Journal of Qualitative Methods, 2(3). Article 3.
Launderdale, M.( 1982 ) Burnout: Strategies for personal and organisational life speculations on evolving paradigm California: university associates
Law M., Stewart D, Pollock N., Letts L., Bosch J & Westmorland M., (1998) Guidelines for critical review from – Quantitative studies. Quantitative review form guidleines1-11
McKenna H (1997) Nursing theories and models New York Routldge
Macnee C L and McCabe S (2008) understanding nursing research using research in evidence-based practice 2nd edition Philadelphia Lippincott William and Wilkins
Melnyk B.M. and Fineout-Overholt .E (2005) Evidence based practice in nursing and health care Lippincott Willains and Wilkins Philadelphia
Murphy F( 2004) Stress Among Nephrology Nurses In Northern Ireland
Nephrology nursing Journal Vol. 31, No. 4, 423-431
Newell and Burnurd (2006) Vital notes for nurses: research for evidence-based practice United Kingdom Blackwell Publishing
Newman and Benz (1998) Qualitative methodology quantitative methodology exploring the continuum Board of trustee USA
Olofsson B, Bengtsson C and Brink E (2003 ) Absence of response : a study of nurses’ experiences of stress in the work place Journal of nursing management (11) 351-358
Polit D F and Beck C T (2006) Essential of nursing research: method of appraisal and utilization of nursing research 6th edition Philadelphia Lippincott Williams and Wilkins
Severinsson E I (2001) conformation meaning and self-awareness as core concept of nursing supervision model Nursing Ethics 8 (1) 36 – 44
Severinsson E I and Kamaker D ( 1999) Clinical nursing supervssion in the work place – effect on moral stress and job satisfaction journal of nursing management (7) 81-90
Todres L and Holloway I (2006) Phenomenological research in Gerrish K and Lacey The research process in nursing 5th edition USA Blackwell publishing
Speziale H S and Carpenter D R (2007) Qualitative research in nursing: advancing the humanistic imperative 4th edition Philadelphia Lippincott and Wilkins
Polit D F and Beck C T ( 2006) Nursing research: generating and assessing evidence for nursing practice 8th edition Philadelphia Lippincott Williams and Wilkins
Patrick K and Lavery J.F (2007) Burnout in nursing Australian journal of advanced nursing vol:24, p43- 47
Potter B (2005) Overcoming burnout 3rd edition Ronin publishing, inc, Oakland.
Paton, N. (2006) Meet your new nurse leaders: Why is Bullying still Rife? Nursing Times 102(48)20-21
Potter,B.( 2005) Job burnout : what is it and what you can do about it? RONIN publishing. Available at [online]:
http://www.docpotter.com/art_bo-summary.html
Accessed on: [ 5th October 2009 ]
Ryan F, Coughlan M and Cronin P ( 2007) step by step guide to critiquing research part 2: qualitative research British Journal of nursing 16(12) 738-744
Regehr C, kjerulf M, Popova S and Baker A J (2004) trauma and tribution: the experiences and attitudes of operating room nurses working with organ donors Journal of Clinical Nursing (13)430-437
Reddy, L.G (2007) Special education teachers: (occupation stress, professional burnout & job satisfaction), New Delhi: Discovery publishing house.
Schaufeli W and Enzmann D (1998) The burnout companion to study and practice : A critical analysis AD Donker Roterdam London
Salmond S and Ropis P.E (2005) Job stress and general well being: A comparative study of medical-surgical and home care nurses MEDSURG nursing vol:14, p301-309
Smit R ( 2005) HIV/AIDS and the work place: perception of nurses in public hospital in South Africa journal of advanced nursing 51(1),22-29
Su S-F, Boore J, Jenkins M, Liu P-E and Yang M-J (2009) Nurses; perception of environmental pressures in relation to their occupational stress Journal of clinical nursing 18, 3172-3180
Tinsley C, and France N.E.M (2004) The trajectory of the registered nurses exodus from the profession: A phenomenology study of the lived experience of oppression International journal of human caring 8(1) 8-12
Toggerson C (2003) Systematic reviews London: University of York
Tang P F , Johansson C, Wadensten B, Wenneberg S and Ahlstrom (2004) Chinese nurses ethical concerns in neurological ward Nursing ethics (14)6 810-824
WHO Library Cataloguing-in-Publication Data Preventing carer burnout: Inter-Mission Care and Rehabilitation Society (IMCARES): (2008) UNAIDS available at: [online]:
http://search.unaids.org/Results.aspx?q=burnout&o=html&d=en&l=en&s=false&x=0&y=0
Accessed on: [24th September 2009]
World health Organisation (WHO), World Health survey:
Abushaikha and Saca-Hazboun (2009), Job satisfaction and burnout among Palestinian nurses Eastern Mediterranean Health Journal Volume 15 No. 1 January-February. Avalable @ [online]:
http://www.emro.who.int/publications/emhj/1501/article22.htm
Accessed on: [21st October 2009]